 RU
RU
 UA
UA
Overview of Multiple Sclerosis as a Neurodegenerative Disease
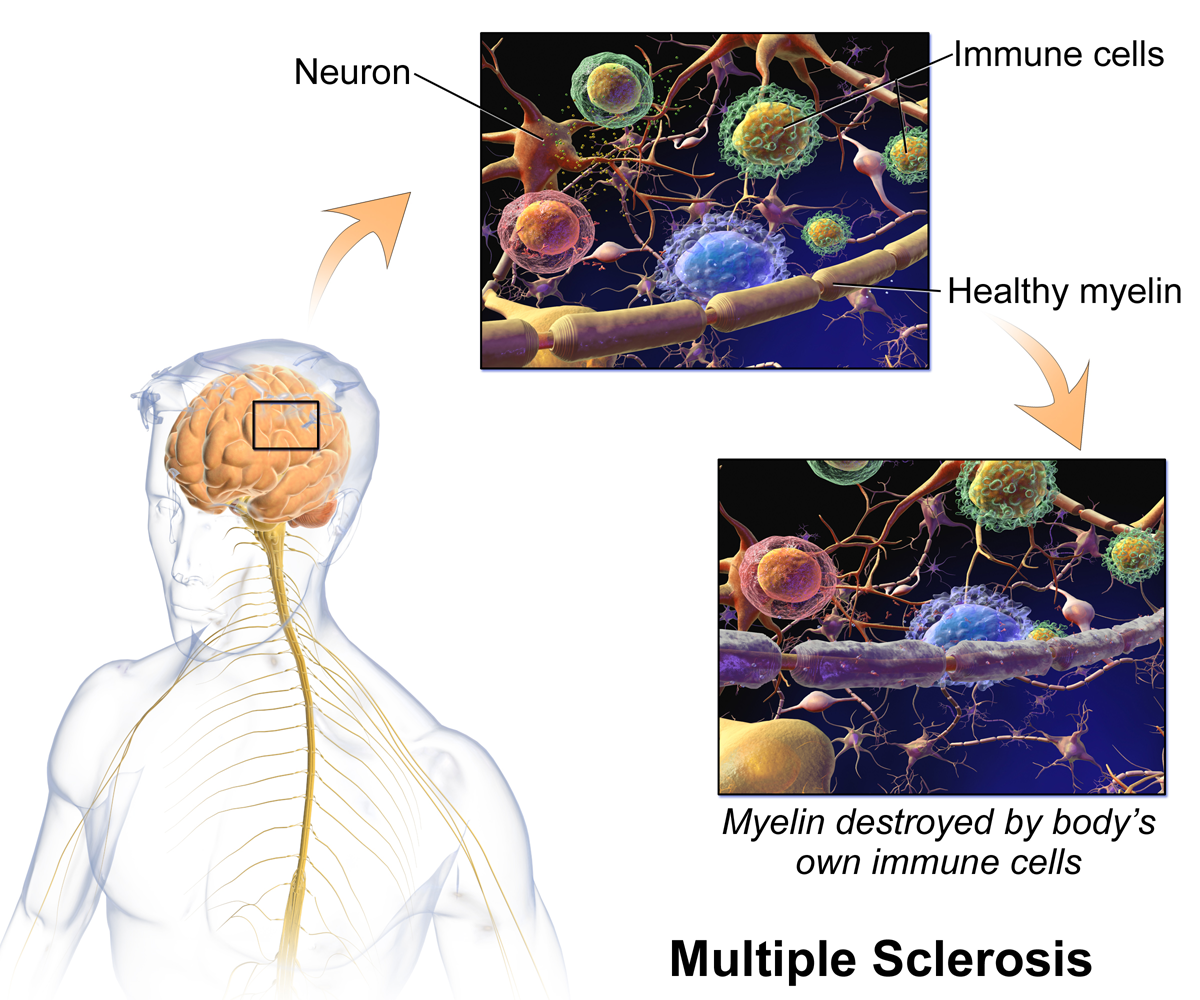
Multiple sclerosis (MS) is a chronic disorder of the central nervous system driven by immune-mediated inflammation, progressive demyelination, and cumulative neuroaxonal injury. The condition affects the brain, spinal cord, and optic nerves, disrupting signal transmission and leading to a broad spectrum of neurological symptoms. These may include fatigue, muscle weakness, sensory loss, impaired coordination, visual disturbances, and cognitive changes.
At its core, MS involves an abnormal immune response directed against myelin—the insulating layer that protects nerve fibers. Repeated inflammatory attacks damage myelin and, over time, the underlying axons. As the disease advances, repair mechanisms become insufficient, resulting in permanent neurological deficits and disability.
While disease-modifying therapies (DMTs) have significantly reduced relapse rates and inflammatory activity, they do not directly restore damaged neural tissue. This limitation has intensified interest in regenerative medicine and stem cell–based strategies that aim to address both immune dysregulation and neural repair.
Why Stem Cell–Based Approaches Are Being Investigated in MS
Conventional MS treatments are largely immunosuppressive or immunomodulatory. Their primary goal is to reduce inflammatory activity, prevent relapses, and delay progression. However, these therapies typically:
- Do not reverse established neurological damage
- Offer limited benefit in progressive MS
- May lose effectiveness over time or cause intolerance
Stem cell–based therapies represent a different therapeutic paradigm. Rather than focusing solely on immune suppression, they are being explored for their potential to combine:
- Immune system recalibration
- Anti-inflammatory signaling
- Neuroprotection
- Support of remyelination
- Improvement of the neural microenvironment
Importantly, “stem cell therapy” is not a single intervention. It encompasses multiple strategies with distinct mechanisms, levels of evidence, and clinical applications.
Hematopoietic Stem Cell Transplantation (HSCT)
The Most Established Cellular Therapy in MS
Autologous hematopoietic stem cell transplantation (HSCT) is currently the best-studied stem cell–based intervention for multiple sclerosis. The procedure involves harvesting a patient’s own hematopoietic stem cells, followed by intensive immunoablation to eliminate autoreactive immune cells, and subsequent reinfusion of the stem cells to reconstitute the immune system.
Clinical Outcomes and Effectiveness
Long-term studies and meta-analyses indicate that HSCT can:
- Induce sustained remission in aggressive relapsing-remitting MS
- Suppress new relapse activity and MRI lesion formation
- Stabilize or improve disability scores in selected patients
In appropriately selected individuals—particularly those with highly active inflammatory disease and shorter disease duration—five-year progression-free survival rates of approximately 60–80% have been reported.
Risks and Limitations
HSCT is a complex and intensive procedure associated with notable risks, including:
- Acute toxicity from conditioning regimens
- Increased susceptibility to infections
- Temporary or permanent infertility
- Treatment-related mortality (now <1% in experienced centers)
Due to these risks, HSCT is generally reserved for patients with aggressive disease who have not responded to standard therapies.
Mesenchymal Stem Cells (MSCs): Immunomodulation and Neuroprotection
A Less Invasive Regenerative Strategy
Mesenchymal stem cells (MSCs) are among the most widely studied cell types in MS outside of HSCT. They can be derived from bone marrow, adipose tissue, or perinatal tissues and are valued for their immunomodulatory and neuroprotective properties.
Unlike HSCT, MSC therapy does not involve immune system ablation and is considered significantly less invasive.
Biological Mechanisms
MSCs exert their effects primarily through paracrine signaling rather than direct cell replacement. Their secreted factors may:
- Reduce pro-inflammatory cytokine activity
- Promote regulatory immune cell populations
- Support oligodendrocyte survival
- Protect neurons from oxidative and inflammatory stress
Current Clinical Evidence
Early-phase trials and observational studies suggest that MSC therapy is generally well tolerated and may:
- Reduce inflammatory activity in some patients
- Improve fatigue and quality of life
- Stabilize disease progression in subsets of individuals
However, results remain variable, and large randomized controlled trials are still ongoing. At present, MSC therapy is best described as promising but investigational for MS.
The Unmet Need: Neuroprotection and Remyelination
Long-term disability in MS is driven not only by inflammation, but by chronic demyelination and axonal degeneration—particularly in progressive forms of the disease. Adult central nervous system repair capacity is limited, and spontaneous remyelination often fails over time.
Stem cell–based approaches may support remyelination indirectly by:
- Activating endogenous oligodendrocyte precursor cells
- Reducing inhibitory inflammatory signaling
- Improving metabolic and vascular support for neural tissue
Even partial preservation of neural networks may translate into meaningful functional benefits.
Induced Pluripotent Stem Cells (iPSCs) and Future Directions
What Makes iPSCs Unique?
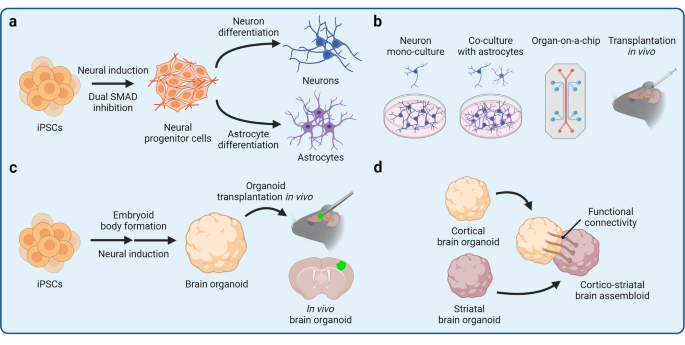
Induced pluripotent stem cells (iPSCs) are generated by reprogramming adult somatic cells into a pluripotent state. They can theoretically differentiate into any neural cell type, including:
- Oligodendrocyte precursor cells
- Mature oligodendrocytes
- Neurons and supportive glial cells
Potential Advantages in MS Research
iPSC technology enables:
- Patient-specific cell modeling
- Reduced risk of immune rejection
- Precise study of disease mechanisms
- Development of personalized regenerative strategies
Current Status
Most iPSC-based MS research remains preclinical. Experimental models have shown that iPSC-derived oligodendrocytes can myelinate axons, but widespread clinical application is likely several years away due to safety, scalability, and regulatory challenges.
Exosome- and Neurotrophin-Based Regenerative Strategies
Overcoming the Blood–Brain Barrier
One of the greatest challenges in MS treatment is delivering regenerative signals across the blood–brain barrier (BBB). Neurotrophic factors such as brain-derived neurotrophic factor (BDNF) play a critical role in neural survival and remyelination, yet cannot effectively cross the BBB when administered systemically.
Exosomes as Biological Delivery Vehicles
Exosomes are nanoscale extracellular vesicles capable of crossing the BBB with high efficiency. When derived from stem cells, they can carry:
- Neurotrophins
- Regulatory microRNAs
- Proteins involved in oligodendrocyte differentiation and myelin repair
This approach enables targeted delivery of regenerative signals directly to demyelinated regions of the central nervous system.
Molecular Targets of Remyelination
Effective remyelination requires coordinated activation of multiple pathways. Exosome-based strategies aim to support:
- OPC activation (NG2/CSPG4 expression)
- Lineage progression and maturation (Olig2 signaling)
- Structural myelin protein restoration (MBP, MOG expression)
Neurotrophin signaling through PI3K/Akt and MAPK/ERK pathways further supports oligodendrocyte survival and myelin synthesis.

Biological Changes Observed After Stem Cell–Based Interventions
Across different stem cell strategies, several consistent biochemical and immunological effects have been reported:
- Reduced autoreactive T and B cell activity
- Increased regulatory T cell populations
- Decreased pro-inflammatory cytokines
- Lower microglial activation
- Stabilization of neurofilament light chain (NfL) levels
These changes help explain why some patients experience disease stabilization or functional improvement.
Patient Selection and Realistic Expectations
Stem cell therapy is not appropriate for all individuals with MS. Outcomes depend on:
- Disease subtype (relapsing vs progressive)
- Duration of disease
- Degree of irreversible neuroaxonal loss
- Current inflammatory activity
- Overall medical condition
Stem cell–based approaches are not cures, but may offer meaningful benefit in carefully selected patients as part of a comprehensive treatment strategy.
The Future of Regenerative Therapy in MS
Future developments are likely to focus on:
- Combination approaches (immune reset plus neuroprotection)
- Biomarker-guided patient selection
- Advanced cell engineering and exosome technologies
- Integration with rehabilitation and neurotechnology
As research advances, stem cell–based therapies may become part of personalized strategies aimed at slowing progression, preserving function, and improving quality of life.

Conclusion
Stem cell therapy represents one of the most dynamic areas of research in multiple sclerosis. HSCT has demonstrated substantial benefit in selected patients, while MSC-, iPSC-, and exosome-based strategies continue to evolve as potential tools for immune modulation and neural repair.
Responsible clinical application, rigorous research, and realistic patient expectations will be essential to translating these advances into safe and effective therapies for multiple sclerosis.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>