 RU
RU
 UA
UA
Peripheral neuropathy is a widespread neurological disorder that affects millions of people globally and often leads to chronic pain, sensory loss, tingling, and muscle weakness. For many patients, standard medical treatments provide only partial relief or focus solely on symptom control. As a result, regenerative approaches — particularly stem cell–based therapies — are increasingly being explored as potential options to support nerve repair and reduce inflammation.
This article examines peripheral neuropathy from a regenerative medicine perspective, explains how stem cell therapy may work, reviews different neuropathy types, and outlines what patients can realistically expect based on current clinical evidence.
Understanding Peripheral Neuropathy
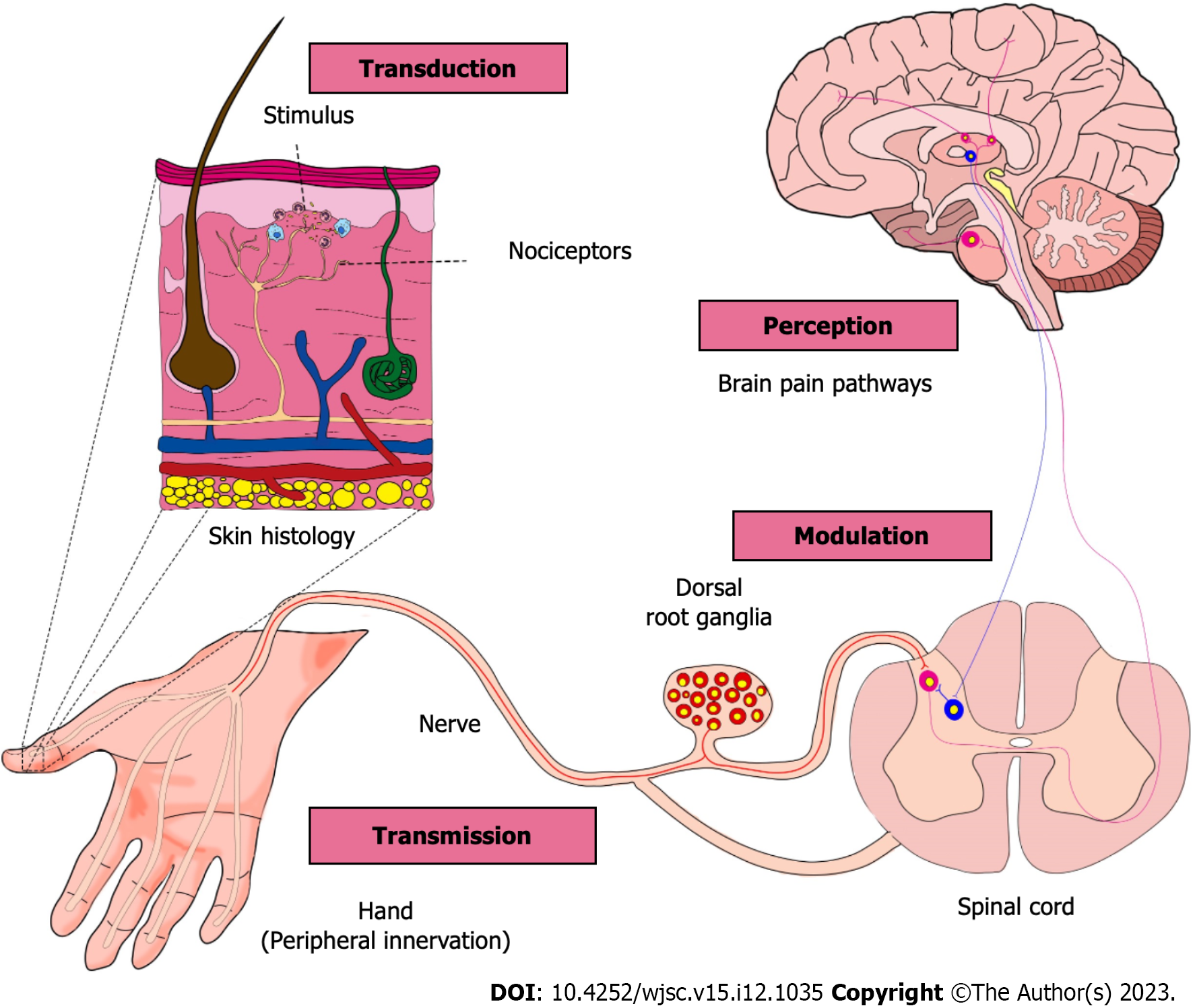
Peripheral neuropathy describes damage or dysfunction of nerves outside the brain and spinal cord. These peripheral nerves are responsible for transmitting sensory, motor, and autonomic signals throughout the body. When they are damaged, communication between the nervous system and organs or muscles becomes impaired.
Common Causes of Peripheral Neuropathy
Neuropathy can arise from a wide range of conditions, including:
* Diabetes and metabolic disorders
* Autoimmune and inflammatory diseases
* Chemotherapy and radiation exposure
* Nutritional deficiencies
* Chronic infections
* Physical trauma or nerve compression
* Idiopathic causes, where no clear origin is identified
Most conventional therapies — such as pain medications, anticonvulsants, antidepressants, and physical therapy — are designed to manage symptoms rather than repair damaged nerves.
Why Regenerative Therapies Are Being Considered
Patients often begin exploring stem cell therapy after experiencing:
* Persistent neuropathic pain that does not respond to medication
* Progressive numbness or sensory loss
* Medication-related side effects
* Minimal functional improvement despite long-term therapy
The interest in stem cell–based treatment lies in its potential to influence the biological environment of damaged nerves, rather than simply suppressing pain signals.
Biological Rationale Behind Stem Cell Therapy for Neuropathy
Stem cell therapy for neuropathy does not aim to replace peripheral nerves directly. Instead, its therapeutic potential is largely attributed to paracrine, immunomodulatory, and neuroprotective mechanisms.
1. Inflammation Modulation
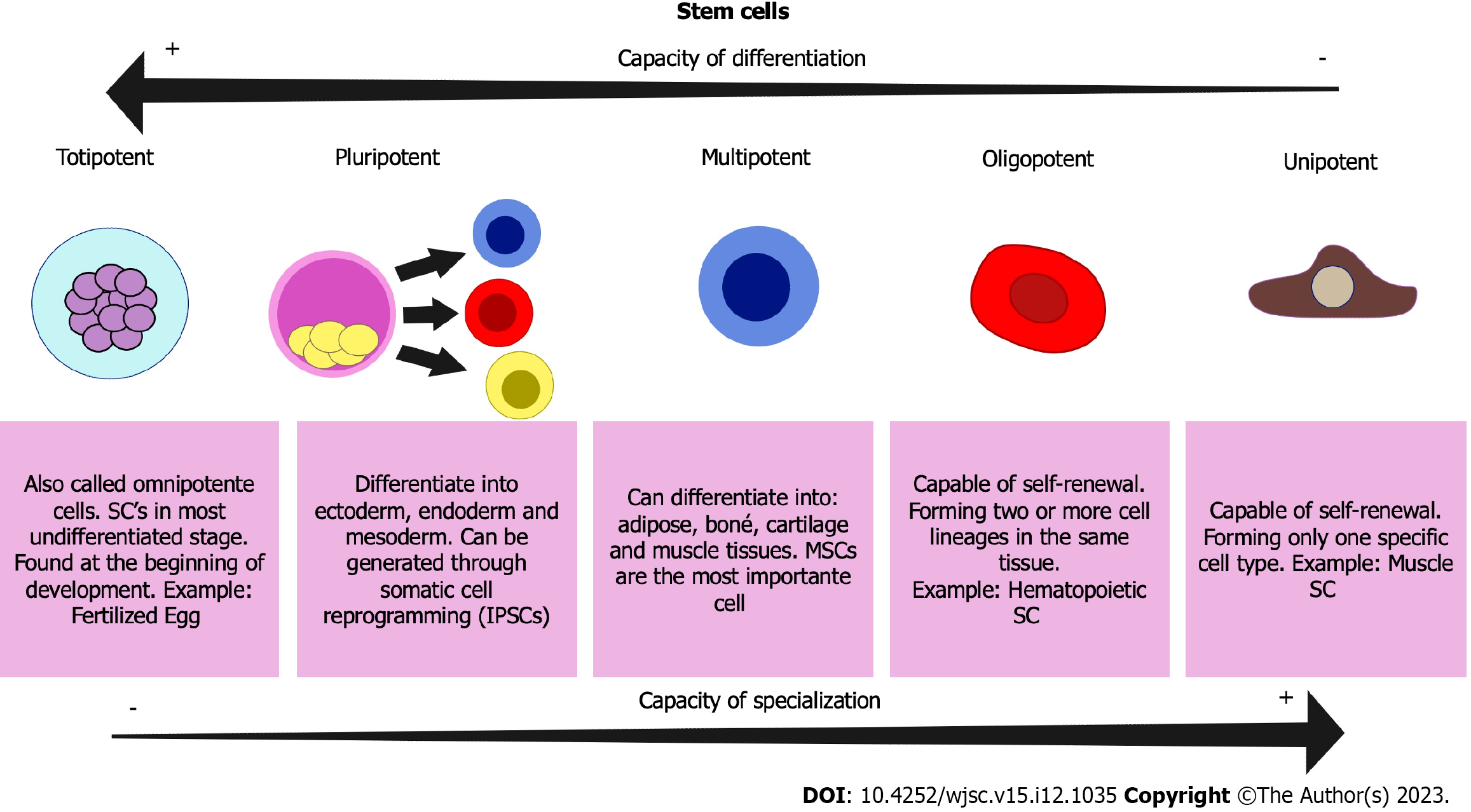
Chronic inflammation is a central contributor to nerve degeneration in many forms of neuropathy. Mesenchymal stem cells (MSCs) are known to regulate immune activity and reduce pro-inflammatory signaling in affected tissues.
2. Neuroprotective Support
Stem cells release a variety of bioactive molecules that may help protect existing nerve fibers from further damage and degeneration.
3. Paracrine Signaling and Tissue Support
Through the secretion of growth factors, cytokines, and signaling proteins, stem cells may:
* Promote axonal support and regeneration
* Improve microvascular circulation
* Enhance local tissue repair
4. Schwann Cell Activation
Schwann cells play a critical role in peripheral nerve repair and myelin regeneration. Stem cell–derived signals may indirectly stimulate Schwann cell activity, supporting remyelination processes.
It is important to emphasize that stem cell therapy is **not considered a definitive cure**, but rather a regenerative support strategy.
Evidence from Clinical Research
Early clinical studies and observational reports suggest that stem cell–based interventions may lead to improvements in pain, sensation, and functional stability in selected neuropathy patients — particularly those with inflammatory or metabolic causes.
However:
* Clinical responses vary widely between individuals
* Large-scale randomized trials remain limited
* Long-term outcomes are still under investigation
For this reason, reputable medical centers classify stem cell therapy for neuropathy as experimental or adjunctive, not guaranteed treatment.
Stem Cell Strategies by Neuropathy Type
Diabetic Neuropathy
Diabetic neuropathy is the most prevalent form of peripheral neuropathy and is strongly associated with microvascular dysfunction and chronic inflammation. Most regenerative protocols focus on MSCs due to their anti-inflammatory, angiogenic, and neuroprotective effects. In some advanced approaches, endothelial progenitor cells (EPCs) are explored to address vascular insufficiency that contributes to nerve damage.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
CIPN results from direct neurotoxic injury to sensory neurons. Treatment strategies emphasize neuroprotection and paracrine support rather than structural nerve replacement. MSCs, as well as MSC-derived exosomes or neural secretomes, are being investigated to reduce neuroinflammation and support neuronal survival.
Autoimmune-Associated Neuropathy
Neuropathies linked to autoimmune diseases are primarily driven by immune-mediated nerve injury. MSCs are particularly attractive in these cases due to their immunomodulatory properties, which may help reduce ongoing immune attacks on peripheral nerves.
Idiopathic Neuropathy
When no clear cause can be identified, treatment strategies tend to be broad and supportive. MSCs are commonly used for their wide-ranging paracrine effects, with goals focused on symptom stabilization and quality-of-life improvement rather than targeted correction.
Traumatic and Compression-Related Neuropathy
Localized nerve injury caused by trauma or chronic compression may benefit from regenerative strategies that support Schwann cell activity and axonal guidance. Experimental studies are investigating MSCs with Schwann cell–like properties, though these approaches remain investigational.
Small Fiber Neuropathy
Small fiber neuropathy affects thin sensory fibers responsible for pain and temperature sensation. Because direct replacement is not currently feasible, stem cell approaches focus on reducing inflammation and providing neurotrophic support through paracrine signaling.
Advanced and Combination Regenerative Approaches
Neural Stem Cells
Neural stem cells (NSCs) are lineage-specific cells capable of differentiating into neurons and glial cells. Their use is primarily limited to controlled research settings and severe cases due to their specialized nature and higher complexity.
Endothelial Progenitor Cells
EPCs target the vascular component of neuropathy by promoting angiogenesis and improving tissue perfusion, especially relevant in diabetic and ischemic neuropathies.
Exosomes and Cell-Free Therapies
Exosomes derived from stem cells contain growth factors and microRNAs that mediate many regenerative effects. Combination approaches using stem cells and exosomes aim to enhance therapeutic signaling while minimizing cellular risks.
Mitochondrial and Metabolic Support
Emerging research suggests mitochondrial dysfunction plays a role in certain neuropathies. Experimental strategies explore mitochondrial-supportive vesicles derived from stem cells to improve neuronal energy balance.
Safety Considerations
When performed under appropriate medical standards, stem cell therapy is generally well tolerated. Potential risks may include:
* Temporary discomfort or swelling at injection sites
* Rare immune reactions
Patients should be cautious of clinics promising immediate or complete nerve regeneration.
Patient Selection and Expectations
Stem cell therapy may be considered for patients who:
* Have chronic or progressive neuropathy
* Show limited response to standard treatments
* Have stable underlying medical conditions
Earlier stages of neuropathy tend to respond more favorably than advanced axonal degeneration.
Treatment Process and Costs
Typical protocols may include:
* Comprehensive diagnostic evaluation
* Cell sourcing and preparation
* Intravenous or localized administration
* Post-treatment monitoring
Costs vary depending on cell type, number of sessions, and regulatory environment, and are generally not covered by insurance.

Observed Clinical Outcomes
Reported benefits across studies include:
* Reduction in neuropathic pain
* Decreased paresthesia
* Partial improvement in sensory function
Objective nerve conduction improvements are inconsistent, reinforcing the idea that many benefits arise from anti-inflammatory and neuroprotective effects rather than structural nerve replacement.
Follow-up data suggest that improvements may persist for over a year in some patients, though long-term durability remains under investigation.
Conclusion
Stem cell therapy for peripheral neuropathy represents a rapidly evolving area of regenerative medicine with promising but variable outcomes. While it does not offer guaranteed nerve regeneration, it may provide meaningful symptom relief and functional stabilization for selected patients.
A careful, evidence-based approach — including realistic expectations, appropriate patient selection, and qualified medical oversight — is essential when considering stem cell therapy as part of a comprehensive neuropathy treatment strategy.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>