 RU
RU
 UA
UA
Male infertility is a multifaceted medical condition responsible for nearly half of infertility cases globally. Despite advances in diagnostics and assisted reproductive technologies, a substantial number of men fail to achieve meaningful improvement with standard treatments. This limitation has shifted scientific focus toward regenerative medicine, particularly stem cell–based strategies designed to restore impaired spermatogenesis rather than bypass it.
This article provides a structured overview of male infertility classification, examines the real-world effectiveness of established treatment options, and introduces emerging stem cell–based approaches currently under clinical and translational investigation.
How Male Infertility Is Classified
Male infertility is typically categorized according to the biological level at which sperm production or delivery is disrupted. Correct classification is essential for choosing an appropriate treatment pathway.
1. Pre-Testicular Infertility
Pre-testicular causes originate outside the testes and involve hormonal or systemic dysregulation that prevents adequate stimulation of spermatogenesis.
Common factors include:
- Hypogonadotropic hypogonadism
- Hypothalamic–pituitary axis dysfunction
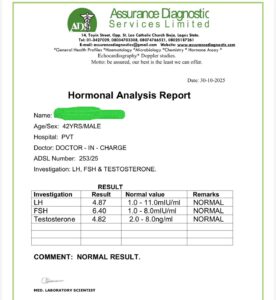
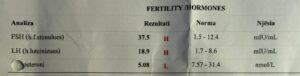
- Abnormal levels of FSH, LH, or testosterone
- Chronic metabolic or systemic diseases
In these cases, the testes may retain intrinsic spermatogenic potential if proper hormonal signaling is restored.
2. Testicular Infertility
Testicular causes arise from intrinsic damage or dysfunction within the testes and represent the most challenging category to treat.
Typical conditions include:
- Non-obstructive azoospermia (NOA)
- Sertoli-cell-only syndrome
- Spermatogenic maturation arrest
- Genetic abnormalities (e.g., Klinefelter syndrome, Y-chromosome microdeletions)
- Testicular injury due to infection, chemotherapy, radiation, or toxins
These conditions directly impair germ cell development and are often resistant to conventional therapies.
3. Post-Testicular Infertility
Post-testicular infertility involves obstruction or dysfunction of sperm transport mechanisms.
Examples include:
- Obstructive azoospermia
- Congenital absence of the vas deferens
- Ejaculatory duct obstruction
- Post-surgical or trauma-related blockage
Spermatogenesis may be normal, but sperm delivery is compromised.
Conventional Treatments: Effectiveness and Limitations
Hormonal Therapy
Hormonal therapy is primarily indicated for pre-testicular infertility caused by endocrine abnormalities.
Clinical effectiveness:
- Restoration of spermatogenesis in ~30–40% of well-selected patients
- Requires prolonged treatment (6–18 months)
- Ineffective in primary testicular failure or genetic disorders
Importantly, hormonal therapy offers little to no benefit for most patients with non-obstructive azoospermia.
Ultrasound and Physical Stimulation Techniques
Low-intensity ultrasound and other physical stimulation modalities have been explored as supportive interventions to enhance testicular blood flow and metabolism.
Clinical evidence:
- Limited and inconsistent
- May improve microcirculation
- Insufficient as a standalone treatment
These methods remain experimental and adjunctive rather than curative.
Testicular Sperm Extraction (TESE / micro-TESE)
TESE and micro-TESE are surgical techniques used to retrieve sperm directly from testicular tissue for IVF/ICSI.
Reported sperm retrieval rates:
- Obstructive azoospermia: up to 50–60%
- Non-obstructive azoospermia: ~10–30% in specialized centers
Key limitations:
- Does not restore natural spermatogenesis
- Invasive, with risks of fibrosis and testicular damage
- Limited utility in Sertoli-cell-only syndrome and severe NOA
TESE is a retrieval technique, not a regenerative therapy.
Stem Cell Therapy: A Regenerative Shift in Male Infertility Treatment
Unlike conventional methods that manage symptoms or extract residual sperm, stem cell–based therapy aims to correct the underlying biological failure of spermatogenesis.
The Central Role of Mesenchymal Stem Cells (MSCs)
Mesenchymal stem cells do not primarily function by differentiating into sperm cells. Their therapeutic value lies in their ability to modify the testicular microenvironment.
Key biological actions include:
- Secretion of growth factors (VEGF, IGF-1, GDNF, SCF)
- Anti-inflammatory and immunomodulatory effects
- Reduction of fibrosis and oxidative stress
- Improvement of testicular microcirculation
Clinical imaging in some protocols demonstrates increased vascular branching in previously atrophic testicular regions within 3–4 months, indicating microenvironmental recovery.


Rebuilding the Spermatogenic Niche
Normal spermatogenesis depends on a highly organized cellular niche composed of:
- Sertoli cells
- Leydig cells
- Extracellular matrix components
- Local cytokines and growth factors
MSCs contribute to niche reconstruction by:
- Supporting Sertoli cell metabolic and signaling functions
- Enhancing pathways that regulate spermatogonial stem cell survival
- Creating conditions favorable for germ cell differentiation
Rather than replacing germ cells, MSCs enable endogenous spermatogonia to resume development when the niche is restored.
Implantation of Spermatogenic Niches into Adipose Tissue
A novel experimental strategy involves implanting engineered spermatogenic niches into adipose tissue.
Why adipose tissue?
- Excellent vascular supply
- High long-term graft survival
- Strong endocrine and paracrine signaling capacity
These constructs may contain:
- Spermatogonial cells
- Mesenchymal stem cells
- Supporting stromal elements
In clinical practice, isolated viable sperm cells have been observed approximately 3–3.5 months after implantation, often used as a second-stage intervention following microenvironment correction.


Seminiferous Tubule Organoids: Advanced Regenerative Models
One of the most cutting-edge approaches in male infertility research is the creation of seminiferous tubule organoids.
These three-dimensional structures are engineered using:
- Mesenchymal stem cells
- Sertoli cells
- Germ cell populations
Advantages include:
- Recreation of native testicular architecture
- Physiological cell–cell interactions
- Controlled germ cell differentiation
- Potential future application in personalized fertility restoration
Due to high cost and technical complexity, organoid-based strategies are typically reserved for refractory cases or genetic conditions requiring pathway bypassing.

Clinical Status and Realistic Expectations
Stem cell therapy for male infertility is:
- Experimental but rapidly evolving
- Most promising for non-obstructive and post-injury infertility
- Unlikely to benefit severe genetic defects affecting germ cell lineage
Potential outcomes include:
- Partial restoration of spermatogenesis
- Improved likelihood of sperm retrieval
- Enhanced testicular tissue health
It is not a guaranteed cure, but a powerful regenerative support strategy.
Conclusion
Male infertility is a biologically complex condition that often extends beyond the reach of conventional therapies. While hormonal treatment, ultrasound stimulation, and TESE remain important tools, they largely manage consequences rather than restore testicular function.
Stem cell–based approaches—particularly those utilizing mesenchymal stem cells—introduce a regenerative framework focused on rebuilding the spermatogenic microenvironment, supporting endogenous germ cells, and advancing toward sophisticated solutions such as engineered niches and seminiferous tubule organoids.
As clinical research progresses, stem cell therapy may become an integral component of personalized, regenerative treatment strategies for male infertility, offering new possibilities where standard methods fall short.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>