 RU
RU
 UA
UA
Autism spectrum disorders (ASD) represent a complex group of neurodevelopmental conditions characterized by impairments in social communication, speech, behavior, and sensory information processing. According to the World Health Organization, the prevalence of autism continues to increase, which is associated both with improved diagnostics and with the influence of genetic, epigenetic, and environmental factors.
Modern approaches to autism intervention include behavioral therapy, speech therapy and neuropsychological programs, as well as pharmacological support for associated symptoms (anxiety, aggression, sleep disturbances). However, all of these approaches do not directly affect the biological mechanisms underlying impaired brain development.
Regenerative medicine, and cell therapy in particular, opens a new direction in understanding and correcting neurobiological disturbances in autism. The use of neural cells, induced pluripotent stem cells (iPSC), exosomes, and intracellular products is aimed at restoring disrupted neural networks, myelination, synaptic transmission, and neuroimmune balance.
Biological basis of autism: what happens in the brain
Modern research shows that autism is not a single disease but rather a collection of conditions with different pathogenic mechanisms. Among the key neurobiological changes are:
- impaired formation and maturation of neural networks;
- atypical synaptic plasticity;
- imbalance between excitatory and inhibitory neurons;
- deficit of axonal myelination;
- chronic neuroinflammation;
- dysfunction of glial cells;
- disturbances of neuroimmune interaction.
These processes are formed at early stages of brain development and may persist throughout life, affecting cognitive, behavioral, and sensory functions.

Why cell therapy is considered a promising direction
Protocols for the use of cell therapy in autism spectrum disorders have been developed and studied for more than two decades within the fields of regenerative medicine and neuroscience. The first clinical observations using stem and neural cells for neurodevelopmental disorders appeared in the early 2000s and were later expanded through the use of induced pluripotent stem cells (iPSC), exosomes, and other cellular bioproducts. These protocols are used mainly within the framework of clinical trials and expanded access programs, with an emphasis on safety, immunological compatibility, and neurobiological rationale.
It is important to note that to date, the FDA and other international regulatory authorities (EMA, NIH, Health Canada) have approved numerous clinical studies within established regulatory procedures (IND, clinical trial authorization). The results of these studies primarily confirm the safety of the approach and also demonstrate potential improvement in certain cognitive, behavioral, and neurophysiological parameters in some patients. For this reason, cell therapy for ASD is considered by the international scientific community as a promising direction that may be applied only within strictly regulated protocols and in combination with traditional correction methods.
Unlike symptomatic approaches, cell therapy is aimed at modifying the cellular and biochemical environment of the central nervous system. Stem cells and narrowly differentiated neural cells are capable of:
- influencing neuroplasticity;
- regulating neuroinflammation;
- supporting myelin restoration;
- improving interneuronal communication;
- activating endogenous recovery mechanisms.
A key advantage is the paracrine effect — cells not only integrate into tissues but also secrete biologically active molecules that influence surrounding neurons and glial cells.
Neural cells in autism therapy
Neurons and axons
Neurons are responsible for information transmission in the brain. In autism, atypical formation of axonal connections is often observed, leading to impaired information processing.
The administration of neural cells contributes to:
- support of axonal growth and stabilization;
- improvement of synaptic transmission;
- restoration of balance between different brain regions.
Oligodendrocytes
Oligodendrocytes form the myelin sheath of axons, ensuring the speed and precision of signal transmission. Deficient myelination is considered one of the factors contributing to sensory overload and cognitive impairment in autism.
Cell therapy contributes to:
- restoration of myelin;
- improvement of neuronal conductivity;
- reduction of sensory hypersensitivity.
Astrocytes
Astrocytes regulate neuronal metabolism, neurotransmitter balance, and protection of nervous tissue. Their dysfunction may enhance neuroinflammation.
Neural cells and exosomes normalize astrocyte function, reducing inflammatory cascades.
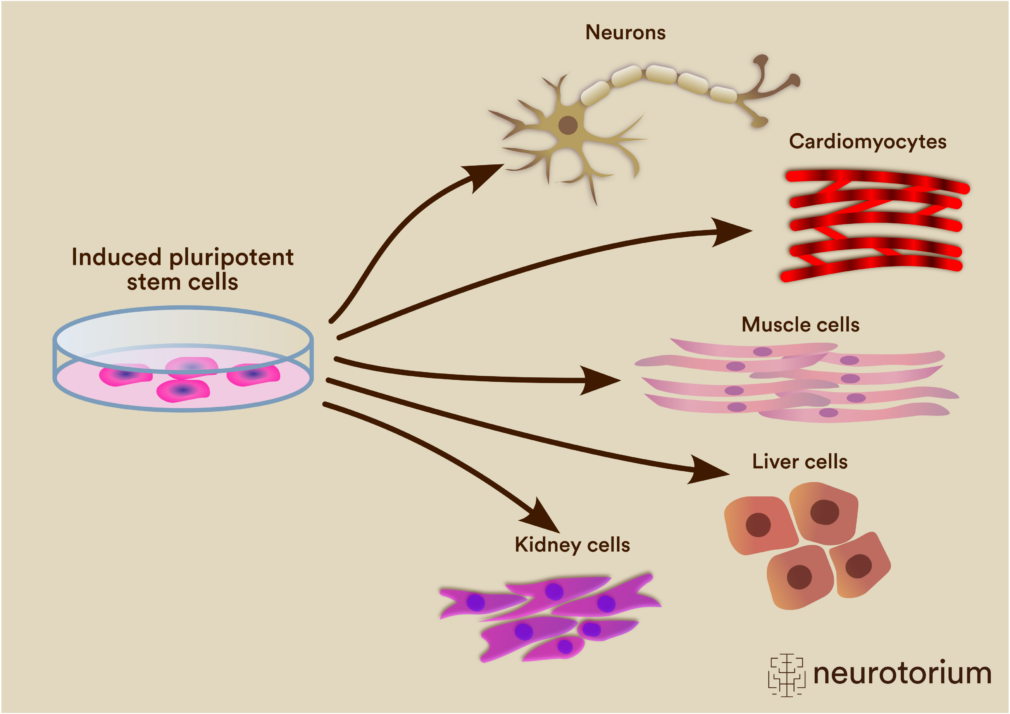
Induced pluripotent stem cells (iPSC)
iPSC are obtained by reprogramming the patient’s somatic cells into a pluripotent state. This allows:
- creation of neural cells taking into account individual genetic characteristics;
- reduction of the risk of immune rejection;
- modeling and correction of neurobiological disturbances.
From iPSC, the following can be derived:
- neurons;
- oligodendrocytes;
- glial cells.
Induced pluripotent stem cells (iPSC) have a number of fundamental advantages compared to mesenchymal stem cells (MSC), especially in the treatment of complex neurobiological conditions such as autism spectrum disorders. The main difference lies in their pluripotency — the ability to differentiate into almost any cell type, including neurons, oligodendrocytes, astrocytes, and other specialized cells of the nervous system. This makes it possible to selectively replenish precisely those cellular populations that are functionally impaired, rather than being limited exclusively to the immunomodulatory and paracrine effects characteristic of MSC. In addition, iPSC can be obtained from the patient’s own somatic cells, which reduces the risk of immune reactions and increases the biological compatibility of the therapy.
Unlike mesenchymal cells, which in most cases act indirectly — through the secretion of growth factors and anti-inflammatory cytokines — induced cells allow more precise modeling and correction of neural networks, restoration of myelination, and synaptic plasticity. This is particularly important in conditions where disturbances in the development and organization of neural connections play a key role. In addition, iPSC make it possible to perform preliminary quality control, genetic screening, and directed differentiation into strictly defined cell subtypes, making the therapy more predictable, personalized, and scientifically grounded compared to the universal use of mesenchymal stem cells.
Exosomes and intracellular products
Exosomes are nanoparticles containing microRNA, proteins, and signaling molecules. They play a key role in intercellular communication.
Exosomes play a key role in modern cell therapy because they are the primary mechanism of intercellular communication through which a significant portion of the regenerative effect of stem and neural cells is realized. These nanoparticles contain biologically active molecules — microRNA, mRNA, proteins, lipids, and signaling factors — that are capable of directly altering gene expression in target cells. In the context of neuroregeneration, exosomes participate in reducing neuroinflammation, regulating synaptic plasticity, supporting neuronal survival, and restoring glial cell function, thereby creating a favorable biochemical environment for the restoration of disrupted neural networks.
An important advantage of exosomes is their ability to cross the blood–brain barrier, which significantly increases the effectiveness of their impact on the central nervous system compared to whole cells. In addition, exosomes do not possess the ability to divide, which reduces the risks of uncontrolled growth and makes their use safer from the standpoint of oncological and immunological complications. Due to their high bioavailability and targeted molecular action, exosomes are considered one of the most promising tools for enhancing and stabilizing the effects of cell therapy, especially in complex neurodevelopmental and neurodegenerative conditions.
After therapy, exosomes:
- regulate gene expression;
- suppress neuroinflammation;
- enhance neuroplasticity;
- improve neuronal metabolism.
Biochemical and cellular processes after therapy
Early phase (first weeks)
- reduction of pro-inflammatory cytokine levels (IL-6, TNF-α);
- improvement of microcirculation;
- stabilization of neurotransmitter balance;
- reduction of neuronal excitability.
Mid-term phase (2–4 months)
- enhancement of synaptic plasticity;
- improvement of myelination;
- normalization of glial cell activity;
- improvement of neuronal metabolism.
Late phase (6–12 months)
- stabilization of neural networks;
- improvement of cognitive and behavioral functions;
- reduction in the severity of sensory disturbances;
- increased adaptability.
Functional recovery after therapy
Clinical observations show improvements in the following areas:
- attention and concentration;
- comprehension and use of speech;
- social interaction;
- reduction of anxiety and stereotyped behaviors;
- improved sleep;
- increased learning ability.
It is important to emphasize that therapy is not a cure for autism but is considered a complementary regenerative approach that enhances the effectiveness of correctional programs.

Treatment outcomes and clinical effectiveness
According to clinical observations and pilot studies, improvements of varying degrees are observed in 60–80% of patients with ASD after cell therapy. The most pronounced changes are observed in reduced hyperactivity, improved attention, decreased sensory overload, and increased social engagement. In young children, the effect is generally more pronounced due to the high neuroplasticity of the brain.
In 40–60% of patients, sustained improvements in speech and cognitive functions are recorded within 6–12 months after therapy. In combination with behavioral and educational correction, cell therapy demonstrates a synergistic effect, allowing the achieved results to be consolidated.
It is important to note that effectiveness depends on many factors: age, severity of ASD, presence of genetic syndromes, comorbid conditions, and individual neurobiological profile. For this reason, a personalized approach is applied.
Patient and parent testimonials
1. Anna, 6 years old, diagnosis: ASD, moderate severity (Poland)
“After the course of therapy, my daughter’s eye contact improved, and more meaningful speech appeared. She became calmer, sleeps better, and learns more easily. After 6 months, the progress is maintained.”
2. Maksym, 9 years old, ASD + ADHD (Ukraine)
“We note a decrease in hyperactivity; the child became more focused and better follows instructions. Behavioral therapy has become much more effective.”
3. Luca, 7 years old, ASD (Italy)
“After treatment, speech comprehension improved and sensory reactions decreased. Teachers at school noted positive changes.”
4. Emily, 5 years old, ASD (Canada)
“The child became more social, engages more often, and sleep improved. We see gradual but stable progress.”
5. Oleh, 11 years old, ASD, severe form (Ukraine)
“Frequent meltdowns disappeared, anxiety decreased, and attempts at communication appeared. It’s not a miracle, but an important step forward.”
6. Jonas, 8 years old, ASD (Germany)
“After therapy, our son became calmer, concentration improved, and he adapts more easily to changes.”
Treatment of autism with stem and neural cells represents a promising direction of regenerative medicine aimed at correcting neurobiological disturbances. With proper selection of cellular products and a comprehensive approach, therapy may contribute to improved quality of life, adaptation, and development of patients with ASD.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>