 RU
RU
 UA
UA
Introduction: Why Heart Failure Still Lacks a Regenerative Solution
Heart failure remains a progressive condition for a substantial proportion of patients, even in the era of advanced pharmacological therapy, cardiac devices, and interventional cardiology. While modern treatment strategies effectively reduce symptoms, hospitalization rates, and mortality, they largely focus on modulating hemodynamic load and neurohormonal activation, rather than restoring damaged myocardial tissue.
At the core of heart failure progression lies a fundamental biological problem: the irreversible loss of functional cardiomyocytes. Once cardiomyocytes are destroyed by ischemia, chronic pressure overload, or inflammatory injury, they are predominantly replaced by fibrotic tissue, resulting in impaired contractility and adverse ventricular remodeling.
This biological limitation has driven increasing interest in cardiomyocyte-based stem cell therapy, a regenerative approach designed to address myocardial cell loss directly. Unlike earlier stem cell strategies that primarily relied on paracrine support, cardiomyocyte-based therapy aims to reintroduce contractile cardiac cells into damaged myocardium, representing a potential shift from symptomatic management toward structural repair.
Heart Failure as a Disease of Cardiomyocyte Deficiency
Regardless of etiology—ischemic heart disease, dilated cardiomyopathy, hypertensive heart disease, or myocarditis—heart failure shares a common cellular trajectory:
- Progressive cardiomyocyte apoptosis and necrosis
- Replacement of functional myocardium with non-contractile fibrosis
- Disruption of excitation–contraction coupling
- Ventricular dilation and declining cardiac output
Adult human cardiomyocytes possess minimal intrinsic regenerative capacity. Estimates suggest that cardiomyocyte turnover in adulthood is insufficient to compensate for injury-induced cell loss, explaining why myocardial damage is largely permanent under physiological conditions.
This recognition has reframed heart failure as not only a functional disorder, but a quantitative deficit of viable cardiomyocytes, providing the biological rationale for cardiomyocyte replacement strategies.

Why Non-Cardiomyocyte Stem Cell Therapies Reach a Biological Ceiling
Early regenerative cardiology trials predominantly investigated mesenchymal stem cells (MSCs) and bone marrow–derived cell populations. These approaches demonstrated encouraging safety profiles and modest clinical benefits, including:
- Reduced inflammation
- Improved microvascular perfusion
- Mild improvements in ventricular function
However, long-term follow-up revealed important limitations. Non-cardiac stem cells do not differentiate into mature cardiomyocytes in vivo and do not integrate electrically with host myocardium. As a result, their therapeutic impact is largely indirect and plateaus over time.
This biological ceiling has redirected research toward cardiac-lineage–specific cell therapies, capable of contributing directly to myocardial contractility rather than solely modifying the surrounding environment.
Cardiomyocytes as a Therapeutic Target in Regenerative Cardiology
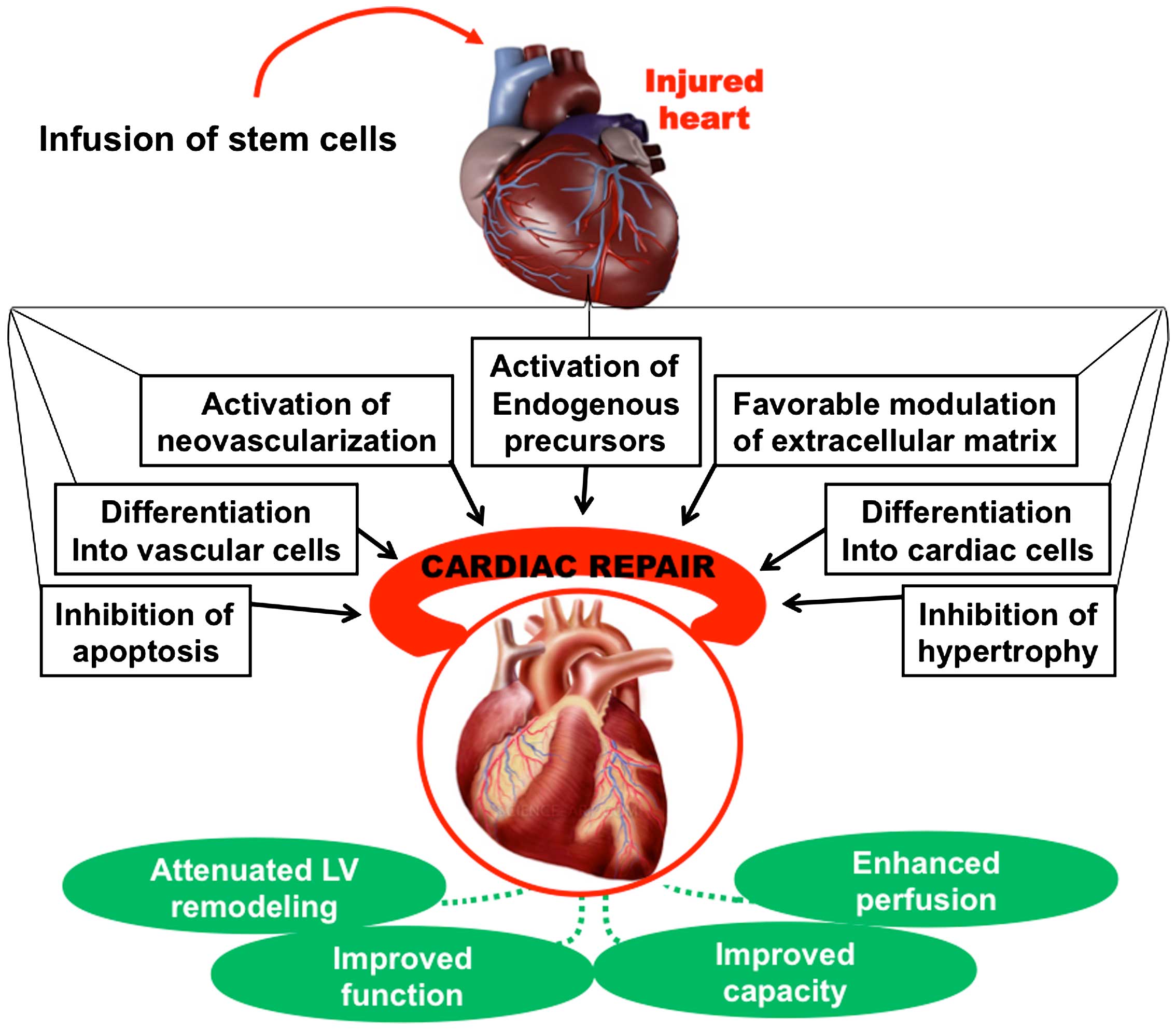
Cardiomyocyte-based therapy represents a conceptual shift in regenerative medicine. Rather than attempting to stimulate endogenous repair mechanisms alone, this approach seeks to replace or supplement lost cardiomyocytes.
Key objectives include:
- Restoring regional contractile units
- Supporting synchronized myocardial contraction
- Reducing adverse ventricular remodeling
- Improving global cardiac performance
The ultimate goal is not complete myocardial regeneration, but partial restoration of functional myocardium sufficient to alter disease trajectory.
Sources of Therapeutic Cardiomyocytes
Induced Pluripotent Stem Cell–Derived Cardiomyocytes (iPSC-CMs)
The most extensively studied source of therapeutic cardiomyocytes is induced pluripotent stem cells (iPSCs). These cells are generated by reprogramming adult somatic cells into a pluripotent state and subsequently guiding them toward cardiac differentiation.
Advantages of iPSC-derived cardiomyocytes include:
- Scalable production of cardiac-lineage cells
- High molecular and structural similarity to native cardiomyocytes
- Potential for autologous or HLA-matched allogeneic use
Challenges remain, particularly related to cell maturation, electrical stability, and immune compatibility, which are active areas of ongoing research.
Embryonic Stem Cell–Derived Cardiomyocytes
Embryonic stem cell–derived cardiomyocytes demonstrate robust differentiation potential and strong contractile properties in preclinical models. However, ethical considerations and regulatory constraints limit their clinical applicability in many regions.
Therapeutic Workflow: From Cell Preparation to Functional Impact
Cardiomyocyte-based therapy is best understood as a multi-stage biological process, rather than a single intervention.
Stage 1: Cardiac Lineage Specification and Maturation
Stem cells undergo tightly controlled differentiation through modulation of key signaling pathways, including Wnt, BMP, and TGF-β. Early cardiomyocytes resemble fetal cells and require further maturation to develop:
- Organized sarcomeric structure
- Functional ion channels
- Effective calcium handling
- Adequate contractile force
Insufficient maturation is associated with arrhythmogenic risk, making this step critical for safety.
Stage 2: Targeted Myocardial Delivery
Delivery methods are selected based on disease distribution and clinical context and may include:
- Intramyocardial injection
- Epicardial patches or engineered cardiac tissue
- Catheter-based transendocardial approaches
Effective delivery maximizes cell retention, regional impact, and integration potential.
Stage 3: Engraftment and Early Survival
Following transplantation, cardiomyocytes encounter a hostile microenvironment characterized by hypoxia, inflammation, and mechanical stress. Engraftment success depends on:
- Adequate vascular support
- Anti-inflammatory modulation
- Protection from apoptosis
Adjunctive strategies such as biomaterials, pro-survival factors, and endothelial co-transplantation are frequently explored.
Stage 4: Electrical and Mechanical Integration
For therapeutic benefit, transplanted cardiomyocytes must:
- Establish gap junctions with host cells
- Synchronize electrical activity
- Contribute mechanically to myocardial contraction
Incomplete integration remains a major challenge and a primary focus of translational research.
Stage 5: Functional Remodeling
When integration is successful, transplanted cardiomyocytes may:
- Improve regional wall motion
- Reduce ventricular dilation
- Stabilize or partially reverse adverse remodeling
- Enhance global cardiac performance
These effects typically evolve gradually over several months.
Supporting Cells and Combination Strategies
Endothelial Cells and Vascular Support
Adequate perfusion is essential for cardiomyocyte survival. Endothelial progenitor cells are frequently investigated as adjuncts to promote angiogenesis and improve long-term graft viability.
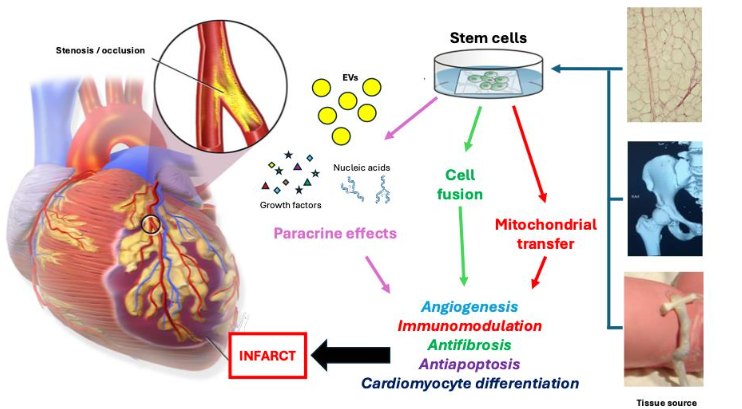
Exosomes and Paracrine Modulation
Stem cell–derived exosomes play an important role in:
- Modulating inflammation
- Enhancing angiogenesis
- Supporting cardiomyocyte survival
- Improving mitochondrial function
Combination strategies using cardiomyocytes and exosomes aim to amplify regenerative signaling while improving safety.
Metabolic and Mitochondrial Support
Heart failure is associated with profound metabolic dysfunction. Experimental research explores whether mitochondrial transfer or metabolic support from stem cell–derived vesicles can enhance cardiomyocyte resilience, although these strategies remain largely preclinical.
Clinical Outcomes and Therapeutic Effectiveness
Early-phase clinical studies and translational trials report measurable but variable functional improvements following cardiomyocyte-based therapy.
Across controlled observational studies:
- Approximately 50–70% of well-selected patients demonstrate clinically meaningful benefit
- Typical improvements include a 5–10 percentage point increase in LVEF
- Symptom improvement often corresponds to NYHA class reduction
Importantly, success is defined as functional stabilization or partial recovery, not complete myocardial normalization.
Duration and Sustainability of Clinical Benefit
Follow-up data suggest that observed improvements may persist for 16 to 48 months in responsive patients. In many cases, benefits stabilize over time, indicating disease modification rather than continuous regeneration. Long-term durability beyond 5 years remains under investigation.
Imaging and Structural Findings
Advanced imaging modalities, including cardiac MRI, have demonstrated:
- Localized improvement in myocardial wall motion
- Modest reduction in scar burden
- Correlation between engraftment and functional outcome
These findings support the importance of cell survival and integration as determinants of long-term benefit.
Variability of Response and Predictive Factors
Response to therapy is highly variable. Favorable outcomes are more commonly observed in patients with:
- Ischemic rather than diffuse cardiomyopathy
- Preserved ventricular geometry
- Limited myocardial fibrosis
- Stable cardiac rhythm
Advanced heart failure with extensive scarring or severe ventricular dilation is associated with reduced response.
Conclusion: Toward Disease-Modifying Therapy in Heart Failure
Cardiomyocyte-based stem cell therapy represents a transition toward disease-modifying strategies in heart failure, addressing the cellular deficit that conventional therapies cannot reverse. While technical and safety challenges remain, this approach offers a biologically targeted framework for myocardial repair in selected patient populations.
As advances in cell maturation, delivery techniques, and patient selection continue, cardiomyocyte-based therapy may evolve from an experimental concept into a defined component of regenerative cardiology.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>