 RU
RU
 UA
UA
Introduction: Why Diabetes Is No Longer Considered Only a Disease of Blood Sugar
Diabetes mellitus is one of the most common chronic diseases of the 21st century. According to the International Diabetes Federation (IDF), more than half a billion people worldwide are currently living with diabetes, and this number continues to increase every year. The disease has long ceased to be regarded solely as an endocrine disorder. Modern science considers diabetes a complex systemic disease affecting virtually every organ and tissue of the body.
For decades, the primary goal of treatment has been the control of blood glucose levels. Insulin therapy, glucose-lowering medications, dietary therapy, and lifestyle modification have significantly increased patients’ life expectancy. However, even perfect glycemic control does not always prevent the development of complications. This is because elevated blood glucose represents only an external manifestation of deeper pathological processes, including chronic inflammation, immune dysregulation, oxidative stress, impaired microcirculation, mitochondrial dysfunction, and the gradual depletion of the body’s own regenerative resources.
For this reason, modern regenerative medicine offers a fundamentally different perspective on diabetes. Instead of focusing exclusively on the symptom—hyperglycemia—researchers aim to target the biological mechanisms underlying the disease by restoring the function of damaged tissues, supporting surviving β-cells, improving the pancreatic microenvironment, and modulating pathological immune processes.
One of the most rapidly developing areas today is cell-based therapy. Particular attention is being focused on mesenchymal stem cells (MSCs), Muse cells, induced β-cells, exosomes, the secretome, mitochondrial support, and other biological technologies that are being investigated as potential tools for restoring damaged endocrine tissue.
It is important to emphasize that most of these approaches are currently at the stage of active clinical investigation. Despite encouraging results from experimental and early clinical studies, large-scale randomized clinical trials are still required to definitively confirm their efficacy and determine the optimal treatment protocols.
Nevertheless, regenerative medicine is now shaping a new paradigm in diabetes treatment, shifting the focus from lifelong disease management toward restoring the body’s own biological function.
Why Diabetes Mellitus Develops
Although type 1 and type 2 diabetes mellitus share one common feature—chronic hyperglycemia—the mechanisms underlying their development differ substantially.
Type 1 Diabetes Mellitus
Type 1 diabetes mellitus is an autoimmune disease.
For reasons that are not yet fully understood, the immune system begins to recognize the β-cells of the pancreatic islets of Langerhans as foreign structures and gradually destroys them.
The principal participants in this process include:
- CD4+ T lymphocytes;
- CD8+ cytotoxic T lymphocytes;
- B cells;
- macrophages;
- dendritic cells;
- pro-inflammatory cytokines.
As β-cells are progressively destroyed, endogenous insulin production declines, resulting in absolute insulin deficiency.
Current research demonstrates that autoimmune aggression begins several years before the appearance of the first clinical symptoms of the disease.
Type 2 Diabetes Mellitus
Type 2 diabetes mellitus has a considerably more complex pathophysiology.
Its development simultaneously involves several processes:
- insulin resistance;
- chronic systemic inflammation;
- mitochondrial dysfunction;
- lipotoxicity;
- glucotoxicity;
- reduced tissue sensitivity to insulin;
- progressive β-cell exhaustion.
Unlike type 1 diabetes, β-cells are initially preserved.
However, the continuous need to compensate for insulin resistance leads to functional overload of these cells.
Over time, the β-cells are no longer able to cope with the increased metabolic demand.
A gradual loss of β-cell function develops.
In the later stages of the disease, many patients also become insulin-dependent.
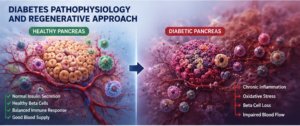
Modern Understanding of Diabetes: A Disease of the Entire Body
Until relatively recently, diabetes was considered exclusively a disorder of carbohydrate metabolism.
Today, such a concept is regarded as overly simplistic.
Modern research demonstrates that diabetes is accompanied by profound alterations affecting virtually every physiological system of the body.
The pathological process includes:
- chronic inflammation;
- immune dysregulation;
- oxidative stress;
- endothelial dysfunction;
- microangiopathy;
- impaired angiogenesis;
- damage to nervous tissue;
- mitochondrial dysfunction;
- impaired intercellular communication;
- reduced activity of the body’s endogenous stem cells.
For this reason, diabetes mellitus is increasingly regarded as a disease characterized by impaired tissue regeneration.
Why Even Perfect Glycemic Control Does Not Prevent Complications
Many patients ask a logical question.
Why do complications continue to develop despite having a good glycated hemoglobin level?
The answer lies in the existence of the so-called metabolic memory.
Even after blood glucose levels have been normalized, many pathological processes continue to persist.
These include:
- chronic inflammation;
- damage to the vascular wall;
- formation of advanced glycation end products (AGEs);
- activation of free radical processes;
- mitochondrial dysfunction;
- progression of tissue fibrosis.
For this reason, modern research is increasingly focused not only on blood glucose control but also on restoring the damaged biology of tissues.
Which Diabetes Complications Are Associated with Impaired Regeneration
Virtually all complications of diabetes mellitus result from chronic tissue damage.
The most common complications include:
- diabetic neuropathy;
- diabetic nephropathy;
- diabetic retinopathy;
- diabetic foot syndrome;
- chronic trophic ulcers;
- cardiomyopathy;
- accelerated development of atherosclerosis;
- chronic kidney disease;
- erectile dysfunction;
- impaired wound healing.
A common characteristic of all these conditions is the reduced ability of tissues to regenerate independently.
This is precisely why regenerative medicine has attracted such considerable interest.
Limitations of Modern Standard Therapy
Over the past two decades, diabetes treatment has advanced significantly.
The following innovations have become available:
- modern insulin analogs;
- insulin pumps;
- continuous glucose monitoring systems;
- GLP-1 receptor agonists;
- SGLT-2 inhibitors;
- combination glucose-lowering therapy.
All of these advances have substantially improved patient outcomes.
However, one fundamental limitation remains.
Virtually none of the currently available therapies are capable of restoring the lost mass of functional β-cells.
Most existing treatments address the consequences of the disease rather than its underlying cause.
Regenerative medicine seeks to target the source of the problem itself—the damaged pancreatic tissue and the disrupted cellular microenvironment.
Why Regenerative Medicine Has Attracted Such Great Interest
Recent years have marked a genuine breakthrough in our understanding of how tissues regenerate.
Until recently, it was believed that stem cells functioned primarily by replacing dead or damaged cells.
Today, this concept has changed considerably.
Most studies demonstrate that the principal therapeutic effect is mediated through paracrine mechanisms—the secretion of a large number of biologically active signaling molecules that modify the behavior of surrounding cells.
For this reason, modern cell therapy is no longer viewed simply as cell transplantation but rather as a biological system capable of regulating regenerative processes.
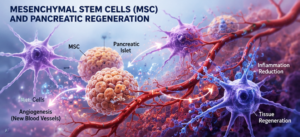
Mesenchymal Stem Cells (MSCs): The Foundation of Modern Regenerative Therapy
Over the past two decades, mesenchymal stem cells (MSCs) have become the most extensively studied cellular platform in regenerative medicine. They were the first cell type to be actively introduced into clinical research involving autoimmune, degenerative, vascular, and endocrine diseases.
Initially, it was believed that MSCs could directly differentiate into the cells of damaged organs, completely replacing destroyed tissues. However, modern research has substantially changed this concept.
It is now understood that the principal therapeutic potential of MSCs is associated not so much with their differentiation but rather with their unique ability to regulate tissue repair through the secretion of a large number of biologically active molecules.
In fact, a mesenchymal stem cell represents a highly organized biological center of intercellular communication.
Following administration, MSCs actively interact with the immune system, vascular endothelium, fibroblasts, macrophages, epithelial cells, and the body’s own endogenous stem cells, thereby modifying their functional state.
For this reason, many experts today describe MSCs not as a building material, but as the “biological conductor” of tissue regeneration.
Why MSCs Are of Interest in Diabetes Mellitus
In diabetes mellitus, several key biological processes become disrupted simultaneously.
These include:
- chronic activation of inflammatory responses;
- impaired microcirculation;
- endothelial dysfunction;
- oxidative stress;
- impaired angiogenesis;
- progressive β-cell loss;
- reduced activity of endogenous tissue stem cells;
- fibrosis of the islets of Langerhans.
MSCs are potentially capable of influencing virtually all of these mechanisms simultaneously.
This explains the tremendous scientific interest in their therapeutic potential.
Experimental studies have demonstrated that following administration, MSCs are capable of secreting hundreds of biologically active factors.
Among the most important are:
- VEGF;
- HGF;
- IGF-1;
- FGF;
- PDGF;
- TGF-β;
- IL-10;
- prostaglandin E2;
- nerve growth factor (NGF);
- various microRNAs (miRNAs).
Each of these molecules participates in a complex regulatory network controlling inflammation, angiogenesis, tissue regeneration, and cellular protection against apoptosis.
The Immunomodulatory Effects of MSCs
MSCs are of particular importance in type 1 diabetes mellitus.
The primary cause of the disease is the autoimmune destruction of β-cells.
The immune system gradually destroys pancreatic β-cells, recognizing them as foreign structures.
MSCs possess pronounced immunomodulatory properties.
Experimental models have demonstrated that MSCs are capable of influencing virtually all of the major cell populations of the immune system.
They regulate the activity of:
- T lymphocytes;
- B lymphocytes;
- dendritic cells;
- natural killer (NK) cells;
- macrophages;
- regulatory T cells (Tregs).
Particular attention has been focused on the ability of MSCs to shift the immune response from a pro-inflammatory state toward a regenerative phenotype.
This is accompanied by decreased production of:
- TNF-α;
- IL-1β;
- IL-6;
- IFN-γ.
At the same time, the synthesis of anti-inflammatory cytokines, including IL-10, is increased.
Such immune modulation is considered one of the most promising approaches for preserving residual β-cell function.
The Effects of MSCs on β-Cells
Another important area of research is the ability of MSCs to support the survival of the remaining pancreatic islet cells.
Experimental models suggest several potential mechanisms through which this effect may occur.
MSCs are capable of:
- reducing β-cell apoptosis;
- decreasing oxidative stress;
- stimulating islet cell proliferation;
- improving local microcirculation;
- promoting angiogenesis;
- creating a favorable regenerative microenvironment.
Together, these effects may contribute to preserving the functional reserve of the pancreas.
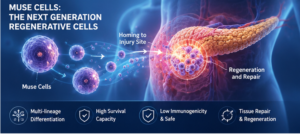
Muse Cells: The Next Generation of Regenerative Biology
One of the most important discoveries of recent years has been the identification of a unique subpopulation of stem cells known as Muse (Multilineage-differentiating Stress-Enduring) cells.
These cells were discovered by Professor Mari Dezawa in Japan and immediately attracted considerable scientific interest because of their unique biological properties.
Unlike most other stem cell populations, Muse cells are a natural component of the human body.
They continuously circulate in the bloodstream in small numbers and become activated following tissue injury.
Research indicates that Muse cells are capable of independently recognizing sites of chronic inflammation and migrating specifically to damaged tissues.
This process is known as homing.
It is believed that Muse cells navigate according to the concentration of specific signaling molecules released by injured tissues.
How Muse Cells Differ from Conventional MSCs
Although Muse cells share certain similarities with mesenchymal stem cells, they possess several unique characteristics.
They are capable of:
- surviving for prolonged periods under conditions of chronic inflammation;
- integrating into damaged tissues;
- differentiating into cells of multiple organs;
- spontaneously ceasing proliferation once regeneration has been completed;
- exhibiting an extremely low risk of uncontrolled growth.
For these reasons, Muse cells are considered a highly promising platform for the regeneration of chronically damaged tissues.
In diabetes mellitus, the principal interest lies in their potential role in restoring both the pancreatic islet apparatus and the vascular network.
It should be emphasized that these mechanisms remain under active investigation and have not yet become part of routine clinical practice.
β-Cell Therapy: Is It Possible to Restore Endogenous Insulin Production?
One of the most ambitious goals of modern regenerative endocrinology is the restoration of the lost β-cell population.
These cells are responsible for insulin synthesis and regulation of blood glucose levels.
In type 2 diabetes, β-cells gradually become exhausted, whereas in type 1 diabetes the majority of β-cells are destroyed by the immune system.
In recent years, several technologies have emerged that aim to address this problem.
The most actively investigated approaches include:
- transplantation of pancreatic islets;
- generation of β-cells from induced pluripotent stem cells (iPSCs);
- differentiation of mesenchymal stem cells into insulin-producing cells;
- pancreatic organoids;
- tissue engineering of pancreatic islets.
Particularly strong interest has been directed toward technologies capable of generating β-like cells from induced pluripotent stem cells.
These cells are capable of synthesizing insulin and responding to changes in glucose concentration.
Several international clinical trials are already evaluating the safety of these technologies in patients with type 1 diabetes mellitus.
Despite impressive progress, these approaches remain in the clinical development stage and require further investigation regarding their long-term efficacy, safety, and durability of therapeutic effects.
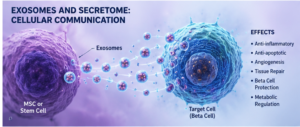
Exosomes: A Biological System of Intercellular Communication
One of the most significant discoveries in modern regenerative medicine has been the realization that the therapeutic effects of stem cells are largely mediated not by their differentiation into new tissue cells, but by the transmission of biological signals to surrounding cells.
The principal mediators of this process are exosomes—microscopic extracellular vesicles measuring approximately 30–150 nanometers in diameter.
Exosomes may be viewed as the body’s natural biological information delivery system.
They are produced by virtually every cell type and contain a complex cargo of biologically active molecules, including proteins, lipids, enzymes, microRNAs, messenger RNAs, and numerous signaling factors.
Upon entering target cells, exosomes are capable of altering cellular behavior by regulating inflammation, tissue repair, metabolism, and cellular differentiation.
Unlike conventional pharmaceutical agents, which typically target a single receptor or biochemical pathway, exosomes simultaneously influence numerous interconnected biological mechanisms, thereby producing a more physiological therapeutic response.
For this reason, exosomes are now considered one of the most promising directions in cell-free regenerative medicine.
How Exosomes May Influence Diabetes Mellitus
The pathogenesis of diabetes involves chronic inflammation, oxidative stress, impaired microcirculation, β-cell loss, and dysregulation of the immune system.
Studies have demonstrated that exosomes derived from mesenchymal stem cells are capable of influencing virtually all of these pathological processes.
Experimental models have shown their potential involvement in:
- reducing the production of pro-inflammatory cytokines;
- decreasing β-cell apoptosis;
- stimulating the formation of new blood vessels;
- promoting angiogenesis;
- reducing oxidative stress;
- restoring endothelial function;
- supporting the survival of pancreatic islet cells;
- regulating the immune response.
Particular attention has been directed toward the microRNAs contained within exosomes.
These small regulatory molecules are capable of controlling the expression of hundreds of genes simultaneously, thereby influencing inflammation, the cell cycle, insulin synthesis, and tissue regeneration.
For this reason, exosomes are regarded as a natural biological system capable of reprogramming damaged tissues.
The Secretome: The Biochemical Library of Regeneration
Another important component of modern cell therapy is the secretome.
The secretome refers to the complete collection of biologically active substances released by living cells during their normal physiological activity.
If exosomes may be viewed as information-carrying transport vehicles, the secretome represents the entire spectrum of molecular signals produced by the cell.
It consists of:
- exosomes;
- extracellular vesicles;
- growth factors;
- cytokines;
- chemokines;
- lipid mediators;
- enzymes;
- microRNAs;
- extracellular matrix proteins.
Modern research demonstrates that the secretome is responsible for the majority of the paracrine effects produced by mesenchymal stem cells.
In essence, the cell functions as a sophisticated biological factory producing a complex cocktail of regulatory molecules.
Why the Secretome May Be Particularly Important in Diabetes
Tissue damage in diabetes develops slowly but continuously.
Persistent inflammation gradually alters the microenvironment of virtually every organ.
Vascular function becomes impaired.
Tissue nutrition deteriorates.
Fibrosis develops.
The regenerative capacity of cells progressively declines.
The biological activity of the secretome is directed precisely toward these pathological processes.
Experimental studies have demonstrated that secretome components may:
- stimulate vascular regeneration;
- support the survival of β-cells;
- reduce chronic inflammation;
- accelerate endothelial repair;
- improve intercellular communication;
- activate the body’s endogenous regenerative mechanisms.
For this reason, recent years have witnessed the rapid development of cell-free therapy, in which biologically active products derived from cells are used instead of transplanting living cells.
Mitochondrial Therapy: Restoring Cellular Bioenergetics
Every cell in the body requires energy.
The principal energy-producing organelles are the mitochondria.
These organelles generate adenosine triphosphate (ATP), which is essential for virtually every biological process.
In diabetes mellitus, mitochondrial dysfunction is considered one of the key mechanisms responsible for disease progression.
Chronic hyperglycemia leads to:
- damage to mitochondrial DNA;
- accumulation of reactive oxygen species;
- reduced ATP production;
- development of oxidative stress;
- impaired cellular respiration;
- activation of apoptosis.
Pancreatic β-cells are particularly vulnerable to energy deficiency because their secretory activity requires exceptionally high levels of energy metabolism.
For this reason, modern regenerative medicine is actively investigating strategies aimed at supporting mitochondrial function.
Experimental studies suggest that improving mitochondrial function may potentially:
- reduce oxidative stress;
- increase cellular resistance to injury;
- support insulin synthesis;
- improve the metabolic activity of tissues;
- decrease inflammatory activity.
It should be emphasized that mitochondrial-based therapeutic approaches for diabetes remain an area of ongoing scientific investigation.
Why Combination Regenerative Protocols Are Considered the Most Promising Strategy
During recent years, researchers have increasingly recognized that diabetes cannot be effectively addressed through a single biological mechanism.
The disease simultaneously affects the immune system, the vascular network, connective tissue, the nervous system, cellular energy metabolism, and pancreatic β-cells.
For this reason, the modern concept of regenerative medicine is increasingly based on multimodal approaches, in which several biological technologies are applied together.
From a scientific perspective, the individual components perform complementary functions.
- Mesenchymal stem cells (MSCs) are regarded as a powerful source of immunomodulation and regulation of inflammation.
- Muse cells are being investigated because of their ability to migrate toward injured tissues and participate in regenerative processes.
- Exosomes provide intercellular transmission of regenerative biological signals.
- The secretome contains a broad spectrum of biologically active molecules that support tissue repair.
- Mitochondrial support is intended to improve cellular bioenergetics.
- β-cell technologies are being investigated as potential methods for restoring the insulin-producing apparatus.
This comprehensive strategy reflects the current understanding of diabetes as a multifactorial systemic disease.
It should be emphasized that these combination protocols currently belong to the field of investigational regenerative medicine. Their safety and potential efficacy continue to be evaluated in both preclinical and clinical studies, and optimal treatment protocols have not yet been established by international clinical guidelines.
Scientific Rationale for a Comprehensive Regenerative Protocol in Type 1 and Type 2 Diabetes Mellitus
As regenerative medicine continues to evolve, it has become increasingly evident that the treatment of a complex disease such as diabetes mellitus cannot be based on targeting a single pathological mechanism. Diabetes is a multifaceted disorder involving immune dysfunction, chronic inflammation, endothelial dysfunction, mitochondrial damage, oxidative stress, progressive β-cell loss, impaired microcirculation, and depletion of the body’s endogenous regenerative capacity.
For this reason, modern research is increasingly adopting the concept of combined regenerative therapy, in which multiple biological technologies act synergistically, enhancing each other’s potential therapeutic effects.
It is important to understand that such protocols remain investigational and continue to be evaluated within the field of regenerative medicine.
Why One Cell Type Alone Is Not Enough
For many years, attempts have been made to restore pancreatic function using only a single cell type. However, research has demonstrated that no individual cell population is capable of simultaneously addressing all of the biological abnormalities involved in diabetes.
For example:
- MSCs effectively reduce inflammation but cannot fully replace functional β-cells.
- β-cells are capable of producing insulin; however, without a favorable microenvironment, their long-term survival is limited.
- Exosomes efficiently regulate intercellular communication but cannot independently generate new tissue.
- Muse cells possess remarkable regenerative potential but likewise require support from an appropriate tissue environment.
- Even perfectly functioning cells cannot maintain long-term activity in the presence of severe oxidative stress and chronic inflammation.
Consequently, the current concept is based not on the use of a single technology but on creating a biological regenerative ecosystem, in which each component fulfills a specialized biological function.
Component One — Mesenchymal Stem Cells (MSCs)
In most contemporary studies, MSCs are regarded as the cornerstone of regenerative therapy because of their potent immunomodulatory and anti-inflammatory properties.
The principal proposed functions of MSCs include:
- reducing chronic inflammation;
- decreasing the production of TNF-α, IL-1β, and IL-6;
- stimulating angiogenesis;
- improving microcirculation;
- protecting β-cells against apoptosis;
- reducing fibrosis;
- restoring the tissue microenvironment;
- supporting endothelial function.
In addition, MSCs actively secrete a broad spectrum of growth factors and extracellular vesicles that create favorable conditions for subsequent stages of tissue regeneration.
Component Two — Muse Cells
Muse (Multilineage-differentiating Stress-Enduring) cells represent a unique population of naturally occurring pluripotent stem cells found in adult tissues.
Unlike most other stem cell populations, Muse cells are capable of spontaneously migrating to sites of tissue injury through the process known as homing.
It is believed that under conditions of chronic inflammation these cells recognize signals released by damaged tissues and selectively accumulate at sites of injury.
Research has demonstrated several potential advantages of Muse cells, including:
- high resistance to inflammatory environments;
- prolonged survival;
- the ability to integrate into damaged tissues;
- participation in vascular regeneration;
- support of cellular regeneration;
- an extremely low risk of uncontrolled proliferation.
For these reasons, Muse cells are regarded as a promising component of future regenerative therapies for chronic diseases.
Component Three — β-Cell Therapy
One of the primary objectives of modern regenerative endocrinology is to restore the population of insulin-producing cells.
Several approaches are currently under active investigation, including:
- generation of β-cells from induced pluripotent stem cells (iPSCs);
- pancreatic islet transplantation;
- pancreatic organoids;
- tissue engineering of the islets of Langerhans;
- generation of functional β-like cells.
The potential objective of these technologies is to replenish the deficit of functional insulin-producing cells.
However, most of these approaches remain in the clinical research phase.
Component Four — Exosomes
Virtually all contemporary studies confirm the crucial role of intercellular communication in tissue regeneration.
Exosomes serve as natural carriers of biological information.
They contain:
- microRNAs;
- messenger RNAs;
- proteins;
- lipids;
- signaling molecules;
- enzymes.
Following uptake by target cells, exosomes are capable of simultaneously altering the activity of numerous genes.
In diabetes mellitus, they may potentially contribute to:
- reducing inflammation;
- protecting β-cells;
- improving microcirculation;
- stimulating angiogenesis;
- reducing oxidative stress;
- restoring normal intercellular communication.
For these reasons, exosomes are currently regarded as one of the most promising technologies in cell-free regenerative therapy.
Component Five — Mitochondrial Support
Modern endocrinology increasingly recognizes diabetes as a disease of impaired cellular energy metabolism.
Under conditions of chronic hyperglycemia, mitochondria gradually lose their ability to efficiently produce ATP.
The consequences include:
- cellular energy depletion;
- accumulation of free radicals;
- amplification of inflammatory processes;
- acceleration of tissue aging;
- β-cell injury.
Investigational approaches aimed at supporting mitochondrial function are considered one of the potential strategies for increasing tissue resistance to chronic injury.
Why Home Maintenance Therapy Is Considered an Important Part of the Regenerative Process
Tissue regeneration is a prolonged biological process.
Following the administration of cell-derived products, a complex sequence of biological events begins, including:
- cell migration;
- adaptation to the tissue microenvironment;
- remodeling of the immune system;
- formation of new blood vessels;
- remodeling of the extracellular matrix;
- restoration of intercellular communication;
- gradual stabilization of regenerative processes.
These mechanisms continue not for several days but often for several weeks or even months.
For this reason, modern regenerative medicine is increasingly discussing the concept of maintenance biological therapy, the purpose of which is to create a favorable environment that supports ongoing regenerative processes.
Potential investigational components of such a maintenance program may include:
- mesenchymal stem cell secretome;
- exosomes;
- growth factor complexes;
- other cell-derived biologically active products whose safety has been confirmed in appropriate studies.
It is hypothesized that such maintenance therapy may help preserve tissue regenerative activity and prolong the function of regenerative mechanisms. However, both the efficacy and the optimal duration of these maintenance programs require further investigation in controlled clinical trials.
Concept of an Investigational Multimodal Regenerative Protocol
From the perspective of modern regenerative biology, a combined therapeutic strategy may be viewed as a sequence of interconnected biological stages:
Reduction of chronic inflammation and immune dysregulation
(MSCs, immunomodulatory factors).
Restoration of the tissue microenvironment
(secretome, growth factors, exosomes).
Support of cellular energy metabolism
(mitochondrial approaches — investigational).
Stimulation of tissue regeneration and intercellular communication
(exosomes, extracellular vesicles).
Support of the insulin-producing apparatus
(β-cell technologies — as they continue to develop and achieve clinical validation).
Long-term support of regenerative processes
through the use of cell-derived biological products.
This multimodal strategy reflects the modern transition from treating isolated symptoms toward targeting the biological mechanisms underlying disease. It remains an area of intensive scientific investigation and is considered one of the most promising directions in the development of personalized regenerative medicine for diabetes mellitus.
Conclusion
The modern understanding of diabetes mellitus has changed substantially. Today, diabetes is regarded not merely as a disorder of carbohydrate metabolism but as a complex systemic disease characterized by chronic inflammation, immune dysregulation, vascular dysfunction, mitochondrial impairment, and a reduced regenerative capacity of tissues.
Against this background, regenerative medicine offers new therapeutic perspectives by focusing not only on glycemic control but also on restoring the biological mechanisms damaged by the disease. Mesenchymal stem cells, Muse cells, β-cell technologies, exosomes, the secretome, and other cell-derived biological products are being actively investigated as potential tools for supporting tissue regeneration and preserving pancreatic function.
Despite the remarkable scientific progress achieved thus far, most of these technologies remain at the stage of clinical investigation and require further confirmation of their efficacy and safety through large international clinical trials. Therefore, they should currently be regarded as promising investigational approaches rather than replacements for established standard therapies.
Nevertheless, it is already evident that advances in stem cell biology, tissue engineering, and molecular medicine are creating a new paradigm for the treatment of chronic diseases. Over the coming decades, personalized regenerative medicine has the potential to fundamentally transform the management of diabetes mellitus by shifting the focus from lifelong disease compensation toward the preservation and restoration of the body’s own biological functions.



 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>
 " alt="loading" class="img-responsive"/>
" alt="loading" class="img-responsive"/>